ТОР 5 статей:
Методические подходы к анализу финансового состояния предприятия
Проблема периодизации русской литературы ХХ века. Краткая характеристика второй половины ХХ века
Характеристика шлифовальных кругов и ее маркировка
Служебные части речи. Предлог. Союз. Частицы
КАТЕГОРИИ:
- Археология
- Архитектура
- Астрономия
- Аудит
- Биология
- Ботаника
- Бухгалтерский учёт
- Войное дело
- Генетика
- География
- Геология
- Дизайн
- Искусство
- История
- Кино
- Кулинария
- Культура
- Литература
- Математика
- Медицина
- Металлургия
- Мифология
- Музыка
- Психология
- Религия
- Спорт
- Строительство
- Техника
- Транспорт
- Туризм
- Усадьба
- Физика
- Фотография
- Химия
- Экология
- Электричество
- Электроника
- Энергетика
21 страница. If the change in facial form were the result of racial admixture, we should not have the types of deformity patterns that these cases show
|
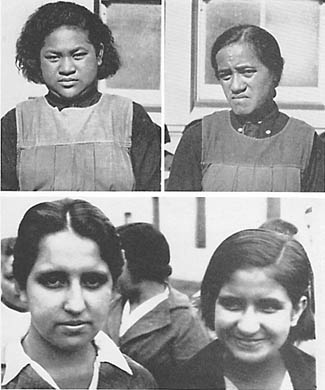
| FIG. 104. Above, two Maori girls in New Zealand and below, two white girls in Peru. Note the facial change in the girls at the right compared with their older sisters. |
If the change in facial form were the result of racial admixture, we should not have the types of deformity patterns that these cases show. Indeed, in the same family we should not find several different deformity patterns. The lack of development downward of the upper anterior incisors and the bone supporting them is illustrated for the younger child, in Fig. 103 lower right. It will be noted that when this girl's molar teeth are in contact her front teeth still miss occluding by a considerable distance.
Members of the white race are affected in a similar manner. In Fig. 104 (lower) are shown two sisters; the younger to the right reveals strikingly the lack of development of the middle and lower third of the face. The fact that this condition so frequently shows a progressively severe injury in the younger members of the family is a matter of great importance in tracing the causative factors. It is important to keep in mind that when the injury shows in the face of the young child it becomes worse when the adult face forms. This increase in deformity occurs at the time of the development of the permanent dentition, at from ten to fourteen years of age.
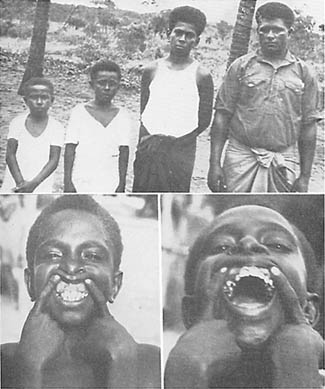
In the islands north of Australia where contact with modern civilization is just being made, the adult individuals showed a constant reproduction of the tribal pattern, while those born since contact was made, had many divergences from normal. In Fig. 105 will be seen a family of six individuals. Four were born before the modern store was put on that island and two after the parents had come into contact with the influence of the imported foods. It will be seen that the four older brothers show marked uniformity of facial design, and that all have reproduced the tribal pattern. The two younger members show definite change in facial pattern. This is also illustrated in Fig. 106 above, in which the oldest brother was born before the store was put on Badu Island, and the three younger, after the establishment of the store twenty-three years ago.

|
| FIG. 105. Of these six brothers the four older were born on Badu Island before the white man's store was established. The two younger at right below, after. Note change in facial form. |
|
| FIG. 106. Above, the brother at the right was born before the store was put on Badu Island, the three younger, after. Note the change in facial form. Below, note that the dental arches are too constricted to provide space for the erupting cuspids. This boy is the one shown at the left in Figure 107. |
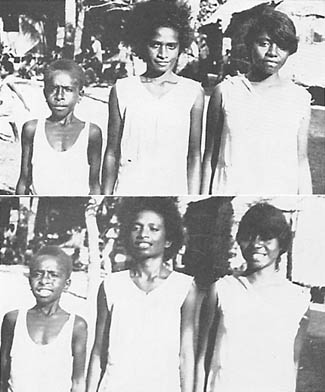
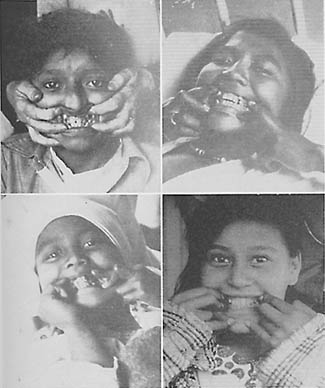
This problem of progressive degeneration in the younger members of the family is again illustrated by the group shown in Fig. 107. The older girl has reproduced the tribal pattern of the race with normal broad, dental arches. The second girl shows marked narrowing and lengthening of the face. The third child, a boy, shows very marked divergence from the tribal pattern. This group is shown below with their teeth exposed. It will be seen that the oldest girl has broad dental arches typical of Nature's normal design. The second girl has a marked depression laterally in the molar and bicuspid region producing a narrowing of the palate. The third child has in addition to the narrowing of the face a marked deficiency in bone growth so that the cuspids both above and below are forced entirely outside the arch. The total circumference as well as the breadth of the upper arch is so reduced that space is not available for the cuspids. They will be seen imbedded high in the tissue, as illustrated in the lower picture of Fig. 106.
|
| FIG. 107. Natives from islands north of Australia. Above, note the progressive facial change in the younger sister and brother with lengthening and narrowing of the face and body. Below, note the broad arches of the oldest girl at the right, lateral depression of the bicuspids and molars of the next girl and inadequate bone development of the boy's face. These are on an island north of Australia. |
Fig. 108 shows three white girl scouts in New Zealand. Note that progressive narrowing of the body including both shoulders and hips has occurred in the younger members of the family. This is also shown in Fig. 107.

|
| FIG. 108. White Girl Scouts, New Zealand. Note the progressive lengthening and narrowing of the face and narrowing of the hips in the younger girl at the left. |
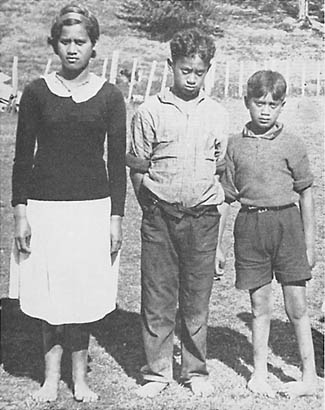
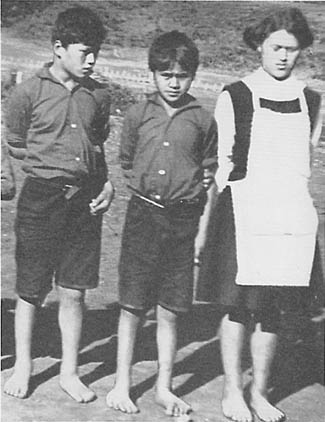
It would be remarkable if these disturbances in the physical pattern were limited to the face and dental arches. An illustration of other deficiency injuries is shown in Fig. 109, which shows three children in a modernized Maori family. It will be seen that while the oldest girl has the typical Maori racial pattern of face, there is a marked lack of development of the middle third of the face, with progressive severity of distortion in her two younger brothers. On observing the feet it will be seen that she has splendidly formed feet while the second child has flat feet, and the third child has clubbed feet.
|
| FIG. 109. New Zealand Mann. Note the progressive change in facial form of the two younger boys as compared with their older sister. Then note the progressive change in their feet. Normal feet, flat feet and club feet. |
I have found similar examples in several of the modernized primitive racial stocks. The severity of the disturbing factors may be different under different circumstances. Drought, industrial depression, unemployment, and the like, all have their influence. In Fig. 110 will be seen three Maori children of New Zealand; the second child is smaller in stature than the third and gives more evidence of facial injury. While his older sister and younger brother have normal feet, his quite severe disturbance in facial growth is associated with club feet.
|
| FIG. 110. New Zealand Maori. Note the marked undersize of the second child and underdevelopment of the face associated with marked deformity of the feet. |
I have one patient who was the seventh of a family of eleven children. All the children in the family have good facial development, except this patient. She was born in the midst of a severe financial depression when the total amount of money available for the food for the family was reduced to a very low level. The other children were born before or after the depression, and were not injured. In addition to this patient's severe facial deformity, she has had some arthritis and a general rheumatic tendency. Her facial injury is marked and is characterized by a lack of development of the middle third.
Deformities of the feet associated with facial deformity have been found in several modernized groups of primitive racial stocks. A typical case among the modernized Indians of Peru is shown in Fig. 111. The face of this boy shows abnormal development with narrowing of the upper arch and displacement of the teeth. This is associated with gross deformity of one foot and shortening of the leg. He lives in the high country. This phase is strikingly illustrated in Fig. 112 where the face is very badly injured and both feet are seriously clubbed. This boy is a Coastal Indian.

|
| FIG. 111. This boy is a modernized Indian in the high Sierra of Peru. Note the disturbed development of the face associated with the deformity of one foot. |

|
| FIG. 112. This is a modernized coastal Indian of Ecuador. Note the serious facial and dental arch distortion associated with club feet. |
The serious expressions of physical deformities which we found had occurred in several primitive racial stocks, after they have become modernized sufficiently to be using the foods of our modern civilization, are occurring in our modern American families with equal severity and great frequency.
One method for determining the cause of these deformities is through an examination of birth and death certificates to note the recorded data relative to physical deformities. An outstanding contribution to this approach has been made by Dr. D. P. Murphy, of the University of Pennsylvania. In an examination of 130,132 individual death certificates that have been recorded between 1929 and 1933, he found physical deformities recorded in 1,476 cases. Dr. Murphy sent field workers to make a personal study of the family histories by contacting the mothers or grandmothers, of whom they were able to locate 890. From this group he was able to select 405 with sufficiently complete family histories to allow tabulation in a form that would throw light upon the birth rank and other data. His studies strongly emphasize the presence of a period of low reproductive activity. In concluding one of his reports he states: (1)
Miscarriages, stillbirths, and premature births occurred more often than would be expected by chance in the pregnancies immediately preceding and immediately following the pregnancy which resulted in the birth of a defective child, and less often than would be expected by chance in the remaining pregnancies. Miscarriage, stillbirth, and premature birth occurred most often in the pregnancy immediately preceding that of the defective child.
From the above observations, it is concluded that the birth of a congenitally malformed child may be only one expression of a prolonged decrease in functional reproductive activity, the other expressions being miscarriages, stillbirths, and premature births.
It is suggested that the obstetrician has unusual reason to suspect the possible existence of a congenital malformation in the pregnancy which follows immediately after a miscarriage, a stillbirth, or a premature birth.
Shute, of the University of Western Ontario, London, Canada, in a personal communication, states that he has been impressed, in his studies of aborted fetuses, with the large percentage that are malformed. This seems to link the malformations with the causative factors which have resulted in decreased reproductive activity.
In connection with the production of imperfect infants, the period in the formative process at which the injury occurs and also its origin are important. Murphy has thrown important light on this phase in his study of the cause of the defectives in forty families with two or more malformed. (2) He concludes: "Many if not most of the congenital malformations met with in this study resulted from defects in the germ plasm, which were present before fertilization."
Among the important questions that arise is the relative responsibility of the two parents. As an approach to this phase Murphy (2) has made a study which deals with a consecutive series of 884 families in each of which there appeared at least one congenitally malformed child. In forty of these families, there were two or more malformed brothers and sisters. He presents extensive data in tabular form from which he takes examples to illustrate his interpretation. He states under the "Clinical Value of Study" the following:
It is evident from the above data (tables) that there is a strong tendency for congenital malformations to duplicate in siblings that belong to a consecutive series of families. And also that such defects tend to appear rather frequently among their more distant relatives. This duplication of malformations is to be observed in the case of the more serious types of defects, just as it is noticed in the less serious ones. These findings lend support to the theory that congenital malformations are primarily the result of influences which affect the germ cells prior to, rather than after, fertilization. The validity of this theory is emphasized by three examples taken from Tables I and II. Family 17 in Table I contained 3 children with pyloric stenosis, two of which were twins. Family 6 in Table II possessed 2 siblings with cleft palate, conceived by the same father, but born to different mothers. Family 8 in Table II contained 2 children both exhibiting an absence of the right half of the diaphragm. It does not seem likely that such sequences of events as these could be the result of any forces that did not operate until after fertilization had taken place....
Since, as has been shown in a previous report, congenital malformations are 24 times more common in siblings of defective children than in the population at large, the present observations should be of added clinical interest.
Summary and Conclusions
1. A consecutive series of 40 families having 2 or more congenitally malformed children has been studied with respect to the duplication of defects in siblings.
2. The defect observed in the first malformed child reappeared in a subsequent malformed sibling in about 50 per cent of all cases; the 50 per cent remaining including all other possible defects.
3. In a second group of 39 consecutive families, in which a malformed child possessed a malformed relative, the malformation in the child and in the relative were identical in about 41 per cent of cases.
4. In 19 non-consecutive families with 2 or more malformed children, the defect of the first child repeated in a subsequent child in over half of the families.
It is significant that while these important factors are just coming to light in our modernized civilization, the evidence clearly indicates that several so-called primitive races have been conscious of the need for safeguarding motherhood from reproductive overloads which would reduce the capacity for efficient reproduction. For example, G. T. Baden (3) in his book "Among the Ibos of Nigeria" states:
It is not only a matter of disgrace but an actual abomination, for an Ibo woman to bear children at shorter intervals than about three years.... The idea of a fixed minimum period between births is based on several sound principles. The belief prevails strongly that it is necessary for this interval to elapse in order to ensure the mother being able to recuperate her strength completely, and thus be in a thoroughly fit condition to bear another child. Should a second child be born within the prescribed period the theory is held that it must inevitably be weak and sickly, and its chances jeopardized.
Similarly, the Indians of Peru, Ecuador and Columbia have been familiar with the necessity of preventing pregnancy overloads of the mother. Whiffen (4) in his book "North-West Amazons" states:
The numbers (of pregnant women) are remarkable in view of the fact that husbands abstain from any intercourse with their wives, not only during pregnancy but also throughout the period of lactation--far more prolonged with them than with Europeans. The result is that two and a half years between each child is the minimum difference of age, and in the majority of cases it is even greater.
It may also be important to note that the Amazon Indians have been conscious of the fact that these matters are related to the nutrition of both parents. Whiffen states that:
These Indians share the belief of many peoples of the lower cultures that the food eaten by the parents--to some degree of both parents--will have a definite influence upon the birth, appearance, or character of the child.
This problem of the consciousness among primitives of the need for spacing children has been emphasized by George Brown (5) in his studies among Melanesians and Polynesians in which he reports relative to the natives on one of the Solomon Islands as follows:
After the birth of a child the husband was not supposed to cohabit with his wife until the child could walk. If a child was weak or sickly, the people would say, speaking of the parents, "Ah, well, they have only themselves to blame."
These new data have a very important bearing on the problems of degeneration in our modern civilization. Since it is true that a racial pattern can be changed in a single generation our modern concept and teaching with regard to the role of heredity must be modified, in its relationship to cause and effect. A deformity arising from intercepted heredity is just as truly biologic as a deformity arising from accumulated impacts as expressed in heredity. Instead of blaming the past generations for the distortions or frailties of our modern generation and thus relieving our own generation of responsibility these new data indicate that the social organization that is creating these divergencies from normal must alone accept the responsibility.
This completely changes some aspects of the theories and practice of modern social education. Instead of planning the care and management of distorted personality as though the lesion were the result of environmental influences upon a normally organized individual, it should be looked upon as a distortion affecting one link in the chain of heredity which is neither the result of the distortions of previous links nor a controlling factor for future links in the chain. The prognosis, in other words, while being bad for the individual is not necessarily bad for his or her descendants.
While many of the individuals who have suffered physical distortions have apparently practically normal brain development we shall see in the following chapter that a certain percentage have so great a disturbance in brain organization that they cannot and should not be considered as individually responsible for their behavior.
It is urgent therefore that the data presented in this chapter be looked upon as an important key to the progressive degeneration that is taking place in many parts of the world under the influence of our so-called modern civilization. It is a matter of profound significance that the most primitive races were originally able to avoid the physical degeneration so general in many communities today. It is also a matter of importance that the primitives recognized not only these dangers but were conscious of and practiced adequate means for preventing them. They had sufficient character to achieve the ends which they deemed essential. Weakness in character may constitute the greatest barrier in the reorganization and conservation of our modern civilization.
Two serious defects from which many individuals in our modernized civilization suffer are impacted teeth and the absence of teeth due to their failure to develop. It is significant that in the arches of the primitive races practically all teeth form and erupt normally, including the third molars. In the modernized primitives and among our modern whites with deformed dental arches many teeth are impacted and often several of the permanent teeth have never formed. The evidence indicates that this, like the facial and dental arch deformities is due to an absence of vitamin A in the diet of the mother during the gestation period or of one or both of the parents prior to conception. The cause is discussed in the next chapter.
REFERENCES
1. MURPHY, D. P. Reproductive efficiency and malformed children. Surg. Gynec. and Obst., 62:585, 1936.
2. MURPHY, D. P. The duplication of congenital malformations in brothers and sisters and among other relatives. Surg. Gynec. and Obst., 63:443, 1936.
3. BADEN, G. T. Among the Ibos of Nigeria. Phila., Lippincott, 1921.
4. WIFFEN, T. North-West Amazons. N. Y., Duffield, 1915.
5. BROWN, G. Melanesians and Polynesians. London, Macmillan, 1910.
TABLE OF CONTENTS
Chapter 18
PRENATAL NUTRITIONAL DEFORMITIES AND
DISEASE TYPES
A RELATIONSHIP between physical types and certain disease susceptibilities has been recognized by diagnosticians for centuries. The skill of many physicians in reading intuitively and from external signs the nature of their patients' troubles when these could not be classified with precision played an important part in the successful warfare against disease in the period preceding the advance in modern laboratory technique. For many of the old-time physicians, these constitutional qualities were expressed as diathesis. An individual would be recognized as having a phthisical diathesis (a susceptibility to tuberculosis). Similarly, the arthritis group had a rheumatic diathesis. While modern science has undertaken to express its findings numerically, the problem of reducing the diatheses to mathematical formulas has required so many overlappings, that it has been impossible to establish definite limiting boundaries.
In my investigations regarding the types of individuals who develop rheumatic group lesions as a result of dental focal infections, (1) I found that individuals could be divided into very definite groups in which 15.05 per cent with severe lesions belonged to families in which similar disease symptoms had occurred. Evidence was disclosed of a systemic factor that played a controlling role in determining whether or not the individual would be seriously injured from dental focal infections. It became very clear that the soil was quite as important a determining factor as was the type of infection. This finding led me to broaden the scope of my investigations to include a search for control cases that were free from the degenerative processes. I was not able to find these controls in the clinical material afforded by our modern civilization, and therefore extended the search to isolated primitive racial stocks.
Associated with a fine physical condition the isolated primitive groups have a high level of immunity to many of our modern degenerative processes, including tuberculosis, arthritis, heart disease, and affections of the internal organs. When, however, these individuals have lost this high level of physical excellence a definite lowering in their resistance to the modern degenerative processes has taken place. To illustrate, the narrowing of the facial and dental arch forms of the children of the modernized parents, after they had adopted the white man's food, was accompanied by an increase in susceptibility to pulmonary tuberculosis.
In Fig. 113 will be seen four young people, examined in the tuberculosis wards of the Juneau (Alaska) Hospital for Indians and Eskimos. All exhibited marked evidence of prenatal injury. Note the cuspids erupting outside the line of the arch. The teeth of the upper arch of the boy at the upper left, pass inside the teeth of the lower arch. His upper arch is so narrow that even a finger could not be passed between the lateral walls. These pictures had to be taken with short exposures in the poor light of the wards. They reveal, however, the conditions.
|
| FIG. 113. Eskimo children seriously ill in the tuberculosis wards of the government hospital at Juneau, Alaska. They were too ill to be moved to good light for photographing. Every tubercular child in these wards had disturbed facial development and deformed dental arches. The parents were living on modern foods. |
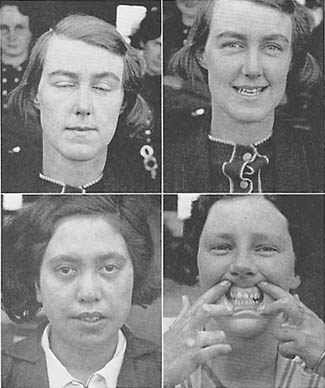
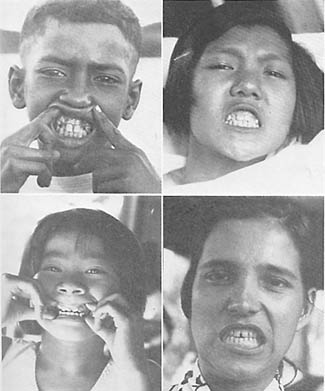
In Figs. 114 and 115 are shown several individuals photographed in the tuberculosis hospital in New Zealand. Note the lack of development of the middle third of the face and the narrowing and lengthening of the face. In several individuals the teeth of the upper arch closed inside the teeth of the lower arch, instead of outside, as in normal persons. Here again, 100 per cent of the young people with tuberculosis gave evidence of injury in the formative period, and 91.2 per cent of the total number of patients were found to have disturbed dental arches.

|
| FIG. 114. These are patients in the Maori Hospital for tuberculosis in New Zealand. Note the very marked underdevelopment of the middle third of the face above and of both middle and lower thirds of the face below. Every patient under thirty years of age in these wards had deformed dental arches and disturbed facial development. |
|
| FIG. 115. These girls are also in the tuberculosis ward of the New Zealand Hospital for Maori. Note the marked disturbance in development of the face and dental arches. All have pinched nostrils. |
In Fig. 116 are shown four typical individuals in the tuberculosis hospitals in Hawaii; one in Hilo and the other in Honolulu. In each of these hospitals 100 per cent of the individuals had abnormal development of the face and dental arches.
|
| FIG. 116. These are native Hawajians in tuberculosis hospitals. Every child in the wards showed marked disturbance of facial development and dental arch form. |
While we know many of the factors contributing to the nature of diatheses, I have found no data dealing with the forces which determine diatheses, except the influence of heredity. The data I am presenting in this volume, deal with forces other than heredity.
An outstanding advance in organizing the data which relate the physical characteristics of individuals to their disease susceptibilities has been made by the Constitutional Clinic of Columbia University and the Presbyterian Hospital of New York, under the able direction of Dr. George Draper. He has found it necessary in order to study man as a whole, to view him from four different angles: "his form, his function, his immunity mechanism and his psychology." These four attributes he has designated as the "four panels of personality." Dr. Draper has published several communications including two textbooks, one entitled, "Human Constitution," (2) and the other, "Disease and the Man." (3) Dr. Draper has approached this problem from the data provided in the medical clinics, and therefore, from the characteristics of affected individuals, whereas my approach has been through a study of the primitive groups and the physical changes and disease susceptibilities which occur as a result of their modernization. The similarity of our conclusions greatly emphasizes the importance of the findings of each. Dr. Draper has emphasized the importance of the face and of the dental arches in the general matter of susceptibility to disease. He closes one of his chapters, entitled The Relation of Face, Jaws and Teeth to Human Constitution and Its Bearing on Disease, as follows:
The lessons which we have learned from these observations, however, is that the face and jaws hold much information of value to the student of the human being. As clinicians in the field of internal medicine we have been taught to observe the gums and teeth in order to detect possible foci of infection. But for the student of clinical organismalism, the teeth and jaws hold much valuable information about the total personality. For the worker in the dental branch of medicine it would seem that an unusual opportunity is offered for extending such observations and correlations. It may very well be that the dental student who becomes interested in the relation of the mouth to the organism may form a most important link with the responsibilities of internal medicine.
The more we come to view man as a totality, as an organism which functions as a whole and not as a collection of separate elements, the more do all the special branches of medicine become fused with the general concept which forms the basis of this discussion, namely, the relation of the human organism as a whole to those various reactions of maladjustment with environment which we call disease.
It is clear that a definite association of abnormal facial patterns with specific disease susceptibilities exists. From my studies it is also clear that these abnormal facial patterns are associated with influences resulting from a change in the nutrition of the parents of the individual. We are at this point concerned with the forces that underlie these phenomena.
Не нашли, что искали? Воспользуйтесь поиском: